
 Share This
Share ThisEditor's Update: This article was first published June 19, 2020. It was most recently reviewed and updated June 6, 2022.
In our Ask a Doc series, we sit down with physicians and other clinical experts, including those at Allegheny Health Network (AHN), for a chat on an important health topic. In this article, we learn about prostate cancer screening with Dr. Herman Singh Bagga, a fellowship-trained urologist, and director of the Center for Men’s Health and Genitourinary Reconstruction at AHN.

Dr. Herman Singh Bagga, a fellowship-trained urologist, and director of the Center for Men’s Health and Genitourinary Reconstruction at AHN
For American men, prostate cancer is the second most common cancer, and second leading cause of cancer deaths. Screening with a prostate-specific antigen (PSA) blood test can catch prostate cancer at an early stage, and the typically slow-progressing disease can often be monitored without requiring invasive treatment. However, some sources, including the U.S. Preventive Services Task Force, describe PSA screening as “an individual decision” rather than recommending it outright.
That last part inspired a feeling I prefer not to have when making health decisions: confusion. Fortunately, I had an opportunity to interview Dr. Herman Singh Bagga, a fellowship-trained urologist, and director of the Center for Men’s Health and Genitourinary Reconstruction at AHN. Here is what I learned.
Don Bertschman (DB): Before we talk about preventive screening, are there symptoms that cause concerns about someone having prostate cancer?
Dr. Herman Singh Bagga (HSB): During early stages, prostate cancer generally does not cause any symptoms. However, all prostates, even non-cancerous ones, can cause urinary symptoms as men age, as the prostate naturally increases in size over time. The most common symptoms of an enlarged prostate are urinary issues, such as weakened urinary stream, needing to strain when urinating, or feeling like the bladder is not emptying completely. With time that might become greater frequency or urgency with urination, feeling a need to rush to the bathroom a lot, and potentially waking up during the night. Since these are most often not symptoms of cancer, but simply of an enlarged prostate, we need other testing to try to catch prostate cancer early.
By screening with the PSA test, we can generally catch prostate cancer before it becomes symptomatic. That’s important, because once prostate cancer is symptomatic, it’s usually at a more advanced stage or has spread. When someone shows up with symptomatic prostate cancer, which is, thankfully, rare, they may have some of those same urinary symptoms, but also blood in the urine or semen, unexplained weight loss, and occasionally lower abdominal pain or pain in the spine or hip. Again, this is rare — I wouldn’t want anyone to worry that back pain equals prostate cancer.
More commonly, the urinary symptoms I mentioned start to manifest in about the same age range that we recommend prostate cancer screening — between age 50 and 55. So if someone comes in to be treated for urinary symptoms, we’ll screen them with a PSA test at the same time.
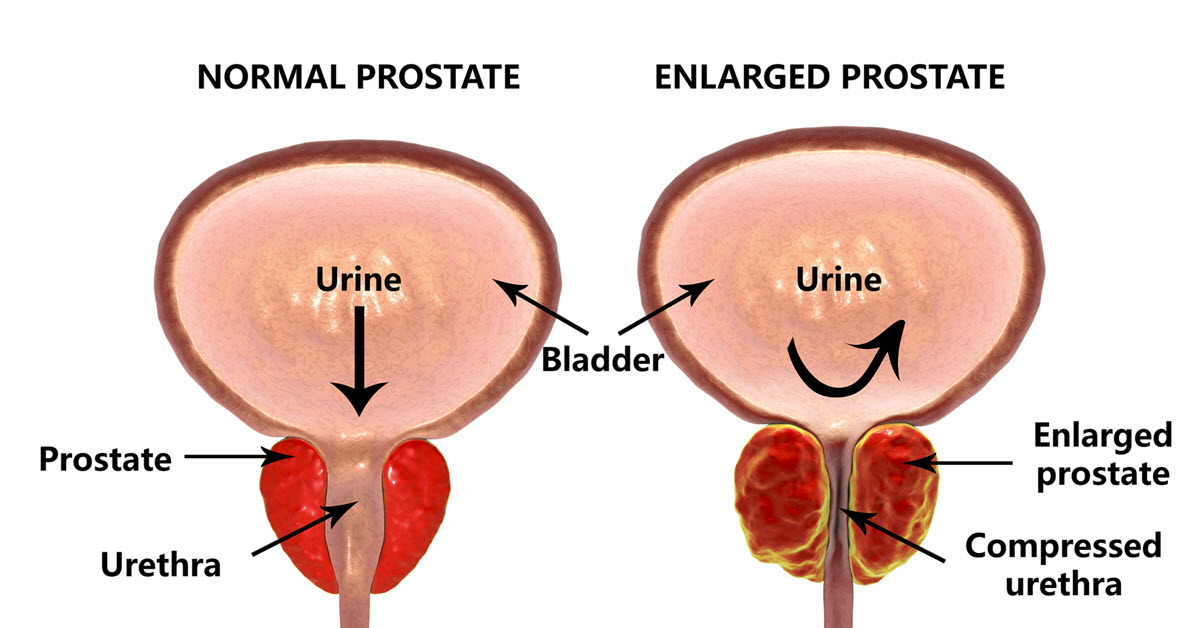
Far more common than prostate cancer, some men develop an enlarged prostate as they get older; the resulting pressure on the urethra and bladder sometimes causes problems with urination.
DB: In 2005, some guidelines shifted away from recommending routine prostate cancer screenings. However, an American Cancer Society study raised concern that now men aren’t screened often enough, with one consequence being a rise in later-stage prostate cancers. Why is there any debate around screening?
HSB: National bodies do vary in recommendations. I personally support the American Urological Association guidelines, which recommend routine PSA screening. We’ll often start at 55 if there are no additional risk factors. With a strong family history of cancer or other risk factors, we start screening closer to 50.
The caveat is that any man we screen for prostate cancer should have a life expectancy of at least 10 to 15 more years. For example, if someone has very severe heart disease, or end-stage cancer, where other providers don’t feel they have a long life expectancy, then we shouldn’t screen for prostate cancer. The reason we look at life expectancy is that prostate cancer is generally a slow-growing cancer. With early-stage diagnosis, a man can go 10, 15 years before it spreads or becomes life-threatening, or even symptomatic. Treatment for prostate cancer has risks, so we wouldn’t treat someone if we didn’t think it would make a difference to their life expectancy and improve their quality of life. If we wouldn’t treat someone, then why screen them in the first place?
Some of the controversy emerged because screening became associated with overtreatment. If the PSA is slightly elevated, that shouldn’t mean an automatic prostate biopsy. Similarly, if a biopsy finds low-grade prostate cancer, that shouldn’t automatically mean invasive treatment such as surgery or radiation. We should never put someone through the undue stress, psychologically and physically, of testing and treatment unless we think that such interventions would improve their quality of life and life expectancy.
Now, personally, I believe the problem is overtreatment, not screening. Done right and responsibly, and using the information intelligently, PSA screening is a simple, powerful tool. But we have to assess each situation, weigh the potential risks and benefits, and make appropriate choices.
DB: That seems like an important distinction — can you walk me through some of the choices and next steps that we’d discuss after a screening?
HSB: Typically, we start with a digital rectal exam to check your prostate for enlargement, or for any abnormalities or nodules that could indicate cancer, and then we also do the PSA test. If there are no abnormalities and your PSA is in the low acceptable range — usually between 2.5 and 4, sometimes increasing a bit with age — we just continue to screen once a year.
If your PSA is borderline, or mildly elevated, first, I recheck it. Then the conversation would include thinking about other causes of PSA rise. That can be as simple as an enlarged prostate, which is a natural part of aging for some men. Any trauma to the prostate can also cause your PSA to rise. I had a patient who was an avid bike rider and rode 100 miles every weekend. All that pressure from the bike on his perineum caused his PSA to be elevated.
But let’s say the PSA is clearly high, or you had abnormalities in the rectal exam. Again, keeping in mind the guidelines about life expectancy, and whether you would be a candidate for treatment, the next step is often a prostate biopsy. The procedure only takes 15 minutes or so in the office. I can usually do it with a person awake, but for those who don’t feel comfortable doing that, we can also do it in the operating room with sedation.
Biopsy samples are the gold standard for evaluating prostate cancer. If the biopsy finds no signs of cancer, then it may be that your baseline PSA is a little higher for a non-cancerous reason. We continue to follow it and see if future PSA tests stay in that same range where we had a normal biopsy. If tests continue to go higher, then we think about another biopsy.
Now, if a biopsy reveals prostate cancer, there’s a very important distinction to be made. We stratify prostate cancer into low risk, intermediate risk and high risk. Intermediate and high risk are where we consider treatment with surgery or radiation. Most of us, including the American Urologic Association and other cancer organizations, now agree that you should not treat low-risk prostate cancer, because it is very unlikely to progress quickly or result in mortality. Instead, we engage in what is called active surveillance — we follow it with regular PSAs and rectal exams, potentially biopsies, and sometimes prostate MRIs. If it goes from low risk to intermediate or high risk, then we discuss treatment. For many men it never progresses beyond low grade, so we can avoid the potential risk of treatment.
DB: Are there any risks or downsides that could lead someone to avoid a PSA or biopsy?
HSB: PSA screening is a simple blood test, so risks or complications are pretty uncommon. However, one risk to keep in mind is that testing is not always reliable. A false positive could take you down the road of an unnecessary biopsy and cause distress physically, but also psychologically. That’s one reason to check with a second test.
I do prostate biopsies regularly, as required, and most people do very well. However, there are risks. When you do a biopsy there is a risk of bleeding. Most men will see a little blood in the urine, stool, or semen, and that can persist for even a few weeks. The most concerning risk is infection. If you have infection at the time of biopsy, that can be a serious event and land you in a hospital requiring broad-spectrum antibiotic treatment. But that’s quite rare — nationally, risk of infection is less than 1% to 3% when you take appropriate precautions. There are also some reported risks of erectile dysfunction after a biopsy. Personally, I’ve never seen that with any regularity, but we let men know it’s a reported risk.
What it comes down to is that we should not proceed with a biopsy, or any procedure, that can have risks unless we’re sure it’s important for a man’s care. PSA risks are low, so if screening is appropriate, that’s an easy recommendation. But a biopsy, I sit down with a man and think through whether to proceed, because we have a little more risk.

When prostate cancer is caught at an early stage, the recommendation is often monitoring rather than invasive treatment. Because the disease usually progresses slowly, many men never get to the point where treatment is needed.
DB: Are there any emerging developments around prostate cancer diagnosis or treatment that you’re excited about?
HSB: Although the technology is not necessarily new, it’s worth mentioning prostate MRIs. Only major centers do these with regularity, and fortunately, AHN has this technology available.
As I said, prostate biopsies are the gold standard for prostate cancer diagnosis, but a prostate MRI can be valuable as an adjunct technology. For example, an MRI might help risk-stratify a man before deciding whether to proceed with a biopsy. Or if a person has a clearly elevated PSA, but a biopsy finds no cancer, a prostate MRI can give us more information. We often use it for active surveillance as well, if we are monitoring a low-risk prostate cancer, to evaluate for signs of progression. Sometimes, a prostate MRI can make the biopsy more accurate; if an abnormality is seen on the MRI, we can use that information to target that area during biopsies.
DB: In a previous interview, you talked about your Center for Men’s Health and the importance of looking at a man’s overall health rather than just a specific issue. Can you talk about how that plays out in terms of prostate cancer screenings?
HSB: We have a few centers for men’s health across AHN now, including in Erie and Monroeville, in addition to the ones I run in Pittsburgh and Wexford. A main goal is making sure that we take care of the whole man and establish a trusting relationship. I take that responsibility very seriously. So, if someone’s immediate concern is erectile dysfunction, for example, I don’t just give them a medication and send them on their way. I will also talk to them about something like prostate cancer screening if appropriate. And vice versa, if someone comes in for a prostate cancer screening, I will make sure to ask about erectile and urinary issues, because I know these are hot-button issues that men would like addressed.
When I see someone, I’m also careful to update their primary care doctor and other relevant physicians with a summary of findings and recommendations so that we can work together to ensure that we take care of the whole man. I also do seminars for primary care doctors and patient groups where we go over issues like erectile dysfunction and prostate cancer screenings.
With the men’s health centers across AHN, we’ve begun to explore how to consolidate services into more of an Institute model. We’re discussing some interesting concepts, like using telehealth as a primary portal of entry to make it easy for men to express their concerns, and then be directed to an appropriate provider near them for in-person follow-up. So that’s another way to think about the whole man and connect him with providers who can handle various men’s health issues, including prostate cancer screening. There are some exciting possibilities, so as that shapes up, that could be a topic for another article.
 Dr. Bagga is a fellowship-trained urologist offering comprehensive medical and surgical care for conditions and diseases of the urinary tract system and male reproductive organs. He has particular clinical interest in genitourinary reconstruction and urethral stricture disease, as well as men’s health issues including sexual dysfunction and Peyronie’s disease. He also specializes in renal stones, benign prostatic hyperplasia, voiding dysfunction and urinary incontinence, and urinary oncology including renal, prostate, penile, and bladder cancers. He has experience in open, laparoscopic, robotic and micro surgery.
Dr. Bagga is a fellowship-trained urologist offering comprehensive medical and surgical care for conditions and diseases of the urinary tract system and male reproductive organs. He has particular clinical interest in genitourinary reconstruction and urethral stricture disease, as well as men’s health issues including sexual dysfunction and Peyronie’s disease. He also specializes in renal stones, benign prostatic hyperplasia, voiding dysfunction and urinary incontinence, and urinary oncology including renal, prostate, penile, and bladder cancers. He has experience in open, laparoscopic, robotic and micro surgery.
Dr. Bagga received his medical degree from Johns Hopkins University School of Medicine in Baltimore, prior to completing residency in urology at the University of California, San Francisco. He then continued training with a fellowship in genitourinary reconstruction and prosthetics at the Cleveland Clinic.
He has authored multiple medical board review published textbooks and has conducted research focused on the epidemiology of disease, surgical techniques, clinical outcomes, and the use of technology in medicine. He serves as editorial board member and reviewer for multiple urologic journals and is a faculty reviewer for McGraw-Hill’s First Aid USMLE Series.
Dr. Bagga has medical staff privileges at Allegheny General Hospital, Allegheny Valley Hospital, Canonsburg Hospital and the Wexford Health + Wellness Pavilion and is welcoming new patients. You can learn more about his approach to health care in this video and hear him talk about men’s urology issues on this KDKA Radio interview.



Highmark Health and its subsidiaries and affiliates comprise a national blended health organization that employs more than 42,000 people and serves millions of Americans across the country.
Entire contents © Highmark Health. All Rights Reserved.
Highmark Health is an independent licensee of the Blue Cross Blue Shield Association.

 Need to find info about providers, prescriptions, coverage, claims, ID cards, or health spending or savings accounts? If so, your Highmark member site is the place to go. (It’s separate from this blog.)
Need to find info about providers, prescriptions, coverage, claims, ID cards, or health spending or savings accounts? If so, your Highmark member site is the place to go. (It’s separate from this blog.)