
 Share This
Share ThisIn our Ask a Doc series, we sit down with physicians and other clinical experts, including those at Allegheny Health Network (AHN), for a chat on an important health topic. In this interview, we talk with Dr. Tom Walsh, medical director of AHN’s Antimicrobial Stewardship Program, about antibiotics and problems created by inappropriate use of antibiotics.
According to the Centers for Disease Control (CDC), “Antimicrobial resistance happens when germs like bacteria and fungi develop the ability to defeat the drugs designed to kill them.”
There’s something cinematic about that scenario — germs and drugs acting out an almost Marvel-esque conflict. However, this conflict has very real societal consequences. The rise of antimicrobial-resistant infections presents a global public health threat that, unlike the average Marvel movie, isn’t guaranteed a happy ending.
I interviewed Dr. Tom Walsh, medical director of AHN’s Antimicrobial Stewardship Program, to learn more about what can be done to meet this challenge, specifically when it comes to the use of antibiotics.

Emily Adamek: Why is antimicrobial resistance a problem we should be concerned about?
Dr. Tom Walsh: The CDC estimates that there are currently around three million antimicrobial-resistant infections in the U.S. every year. Annually, almost 40,000 people die in the U.S. due to these infections — one person every 15 minutes.
Globally, well over a million people die each year from antimicrobial-resistant infections, and it is projected that, if we do nothing, that number will be 10 million deaths a year by 2050 or even sooner.
Emily Adamek: What is driving this rise in resistant infections and the trend toward higher mortality?
Dr. Tom Walsh: By far, the main driver is inappropriate antibiotic use. It’s estimated that 50% of all antibiotic use is inappropriate — it has little or no benefit, and it expands the opportunities for bacteria to develop resistance. 50% — it’s a massive challenge.
Emily Adamek: What are specific examples of inappropriate antibiotic use?
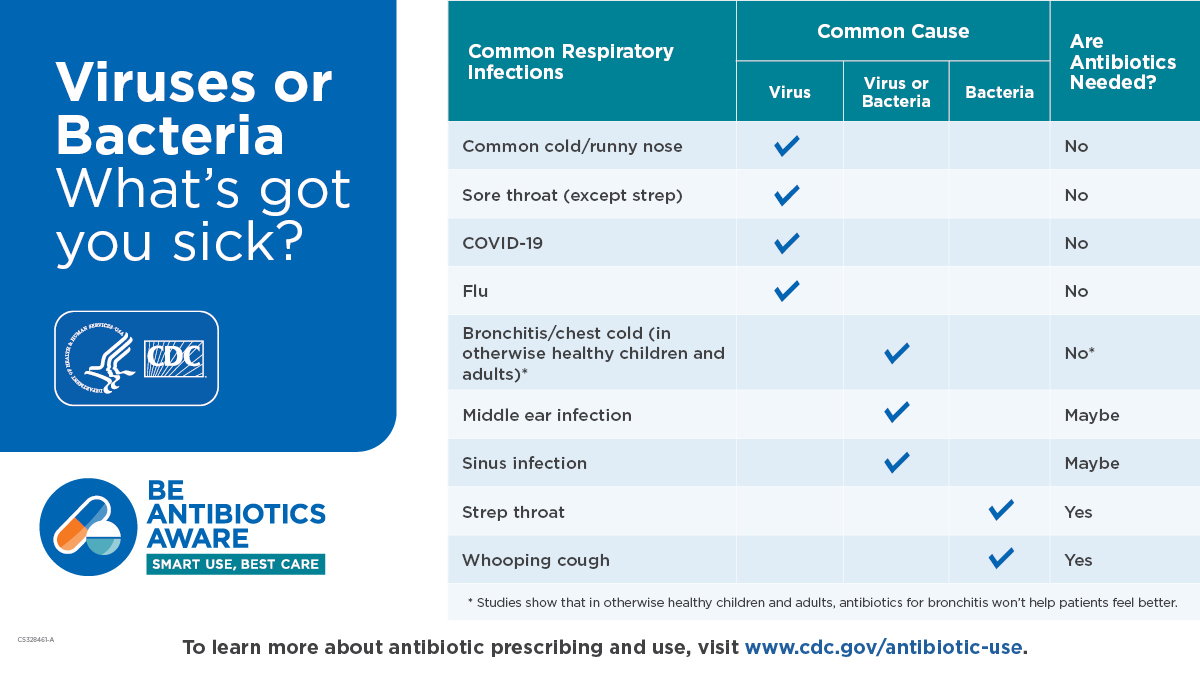
Dr. Tom Walsh: For each disease state, it’s different. Conditions where antibiotics are nearly universally inappropriate include upper respiratory tract infections, acute bronchitis, acute laryngitis, and acute tracheitis. Diagnoses where antibiotics are potentially appropriate include pharyngitis or sinusitis, but there’s criteria for when we should and shouldn’t utilize antibiotics in those cases.
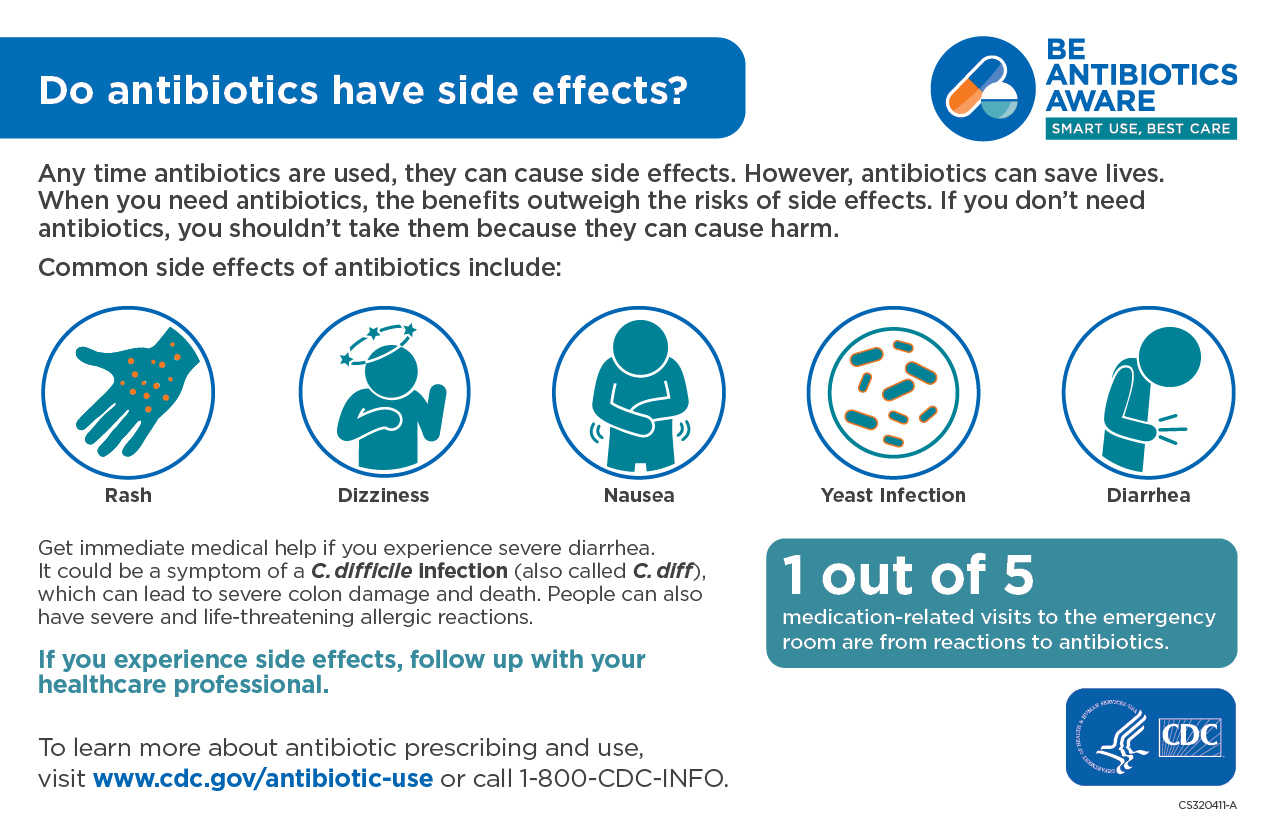
We have good data on when there’s a benefit versus when there is no benefit for using antibiotics. We also need to emphasize the risk side of the equation — unnecessary antibiotic use has potential collateral damage through adverse reactions, increased side effects, and unnecessary costs, as well as the continued propagation of antimicrobial resistance.
Stories and experiences are powerful where sometimes data is not. It can be difficult to wrap your head around facts like 3 million antimicrobial-resistant infections in the U.S. every year. But when you hear stories of patients who developed life-altering C. diff infections, or an infection with a multi-drug resistant organism, that makes the problems real.
Emily Adamek: AHN has a strong antimicrobial stewardship program, and the CDC has many stewardship resources, along with Antibiotic Awareness Week each November. Can you provide a high-level overview of what antibiotic stewardship entails?
Dr. Tom Walsh: Good antibiotic stewardship aims to assist clinicians and patients in maximizing care while minimizing collateral damage associated with antibiotic use.
Historically, most formal efforts to combat inappropriate antibiotic use have taken place in the hospital setting. Unfortunately, that’s just the tip of the iceberg. Hospitals are not where the bulk of antibiotics are used, so we have to shift the target to outpatient settings. That’s not just primary care, but also urgent care, ERs, and outpatient surgical centers.
The risk factors for inappropriate antibiotic prescribing are different in every setting, in every patient population, and within every specialty. Antibiotic stewardship means providing clinicians in each setting with the best information and tools to help them combat the problem. But we also need to do a much better job of explaining the risks of unnecessary antibiotics to patients.
In a hospital setting, the patient is usually not impacting decisions, so there we’re typically focused on misunderstandings among clinicians, as well as some fear and anxiety induced prescribing. The outpatient side is a little different. A lot of outpatient antibiotic use is for disease states where antibiotics are either always inappropriate or often inappropriate. Depending on the disease state, different psychosocial reasons exist for unnecessary antibiotic prescribing, but patient expectations and misunderstandings often play a larger role.
Emily Adamek: Let’s dive into that. What psychosocial reasons would lead to antibiotic overprescribing in outpatient settings?
Dr. Tom Walsh: They are numerous, but often start with basic misinformation. Many people have the idea that every time they have certain symptoms, like a sore throat, they should get an antibiotic. That’s not true. Many people believe that antibiotics can treat viruses. They cannot, they’re only effective with infections caused by bacteria. Another common myth is that if you blow your nose and it’s yellow, that means it’s bacteria, so you should get antibiotics. Again, not true.
So, on the one hand, you have patients who believe they need antibiotics. At the same time, unfortunately, clinicians in outpatient settings are usually remarkably busy. It may take 20 seconds to write an antibiotic prescription and the patient will be satisfied, whereas it would take 20 or 30 minutes of counseling, possibly with the patient getting angry, to explain why antibiotic use is not only not helpful, it’s potentially dangerous. Clinicians need more time and resources.
Emily Adamek: Some people will look at the list of things antibiotics shouldn’t be prescribed for, like head colds or bronchitis, and say they felt better, or their kids got better, after getting antibiotics for these conditions. How do you explain that — is it just placebo effect?
Dr. Tom Walsh: One of the explanations is just math. Many of the viral diseases we’re talking about tend to take 7 to 10 days to improve. Often what happens is that someone tries to ride out the symptoms until day four or five, then they go to a primary care provider or an urgent care. If they receive antibiotics unnecessarily and start to feel better two days later, they think it was the antibiotics, but it was actually because the disease ran its natural course. In reality, they got better in spite of the antibiotics.
There’s a nice quote from Sir William Osler, one of the “Big Four” founding professors of Johns Hopkins Hospital. He said, “The desire to take medicine is perhaps the greatest feature which distinguishes man from animals.”
When you or your kids aren’t feeling well, it’s understandable that you want to do something. It’s hard to hear that you have to wait until something just slowly gets better on its own — especially if you had to take off work and arrange childcare and drive to a doctor’s office just to hear that. So, the way physicians frame the message is important. If you don’t need antibiotics, that’s always good news!
Emily Adamek: A previous article about antibiotics in this digital magazine had a section on penicillin and the problem of mislabeled penicillin allergies. How does that fit in?
Dr. Tom Walsh: AHN has an ongoing initiative to address allergies and presumed allergies to penicillin, which includes a group of antibiotics that are often the safest, most effective choice for a given medical situation.
From 10% to 20% of hospitalized patients have a self-reported penicillin allergy; however, of those, 80% to 90% are not actually allergic. The reason that’s a problem is that if we rule out penicillin because of a mislabeled allergy, then we have to use second-line agents that are typically broader spectrum, less effective, and more costly. For example, one study showed that use of second-line agents for perioperative prophylaxis was associated with a 50% increased risk of surgical site infection, which can be devastating and even life threatening, especially if a patient has a prosthetic knee or hip or hardware in their back.
Emily Adamek: How are you reducing the number of mislabeled allergies?
Dr. Tom Walsh: Through thorough history taking, we can de-label most patients. As I said, most don’t have true allergies. We also know that 80% of people outgrow penicillin allergies within 10 years and are able to safely tolerate it after that. Among those who don’t outgrow it, the overwhelming majority are able to tolerate other “cousins” of penicillin.
In addition to history taking, we use skin testing, as well as oral graded challenges, where we give 10% of an oral dose, monitor for an hour, give the remaining dose and monitor, then transition to IV dose and continue to monitor. We’ve done this successfully for hundreds of patients who we’ve then been able to put on first-line antibiotics.
This is another issue where we are also moving more to the outpatient setting. In other words, we don’t want to wait until someone is in the hospital and we have to decide whether or not to use penicillin, we want to do history taking and penicillin skin testing if necessary in outpatient settings and correct those penicillin allergy labels in the medical record before someone gets to a hospital.
Emily Adamek: Within the Antimicrobial Stewardship Program at AHN, what strategies are used to reduce unnecessary antibiotic prescription?
Dr. Tom Walsh: Successful strategies to reduce unnecessary antibiotic prescribing include communications training, accountable justification, feedback with peer comparison, and public commitment posters and letters that declare the clinician’s commitment to reduce inappropriate antibiotic use in plain language. There have also been antibiotic pledge handouts with the same verbiage as the posters and letters. These can be distributed to patients by the front office staff while they’re in the waiting room.
Additionally, we created stewardship newsletters that are disseminated to our medical staff and trainees with recommendations for common outpatient conditions, including when antibiotics are indicated, what the first-line and second-line agents are, dosage, and duration, as well as adjuvant non-antibiotic options.
Emily Adamek: Tell me more about peer comparison.
Dr. Tom Walsh: We’re able to show clinicians where they stand among their peers in regard to antibiotic prescribing for different disease states. If you see that 95% of your colleagues are writing for antibiotics significantly less than you are, then that’s motivation to take a closer look and refine your prescribing practices.
Several years ago, we had small cohorts where we were looking at inappropriate prescribing. The practices we looked at had attending physicians as well as residents, but the attending physicians didn’t always see the patient with the residents. What’s interesting is that when the internal medicine resident co-managed patients with the physicians, there was a much lower rate of inappropriate prescribing, indicating that attending physicians were modeling appropriate behavior when someone was watching.
That is a positive example of the Hawthorne Effect — performing differently, and in this case better, when someone else is watching. Similarly, we believe this is how peer comparison helps in general.
Emily Adamek: Do you encounter much push-back from clinicians about antibiotic prescribing practices?
Dr. Tom Walsh: We’ve been collecting our own data for quite some time, so no one feels like they’re being unfairly picked on. When you look at data on outpatient physician perception, they usually agree that antimicrobial stewardship is important, they understand that overprescribing is a problem, but they rarely believe that they or their practice are overprescribing. Most physicians find that having the data, including the kind of peer comparison data I mentioned, is helpful in that respect.



Highmark Health and its subsidiaries and affiliates comprise a national blended health organization that employs more than 42,000 people and serves millions of Americans across the country.
Entire contents © Highmark Health. All Rights Reserved.
Highmark Health is an independent licensee of the Blue Cross Blue Shield Association.

 Need to find info about providers, prescriptions, coverage, claims, ID cards, or health spending or savings accounts? If so, your Highmark member site is the place to go. (It’s separate from this blog.)
Need to find info about providers, prescriptions, coverage, claims, ID cards, or health spending or savings accounts? If so, your Highmark member site is the place to go. (It’s separate from this blog.)