
 Share This
Share ThisEditor's Update: This article was first published May 9, 2016. It was most recently reviewed and updated on February 27, 2025. You may also be interested in this 2024 article and video about establishing the Mario Lemieux Center for Heart Rhythm Care.
In our Ask a Doc series, we sit down with physicians and other clinical experts, including those at Allegheny Health Network (AHN), for a chat on an important health topic. In this interview, we’re talking with Dr. Amit Thosani about the risks, causes and treatments for atrial fibrillation.
Atrial fibrillation, sometimes called AFib, is an irregular heart rhythm from the top chambers of the heart. People experiencing AFib — about 12.1 million Americans according to the U.S. Centers for Disease Control and Prevention — often describe it as a fluttering or quivering sensation in the chest.
Amanda Changuris: Dr. Amit Thosani, as a clinical cardiac electrophysiology specialist with Allegheny Health Network, what kind of symptoms do you see in patients diagnosed with AFib?
Dr. Amit Thosani: Patients experience AFib differently; they may have palpitations, heart racing, shortness of breath, fatigue, or a general sense of being unwell. Patients may have some combination of multiple symptoms. There is also a subset of patients who don’t have symptoms, so they may not know they have AFib.
If you’re experiencing symptoms like these, you’ll want to see your doctor so they can help you figure out what’s going on.
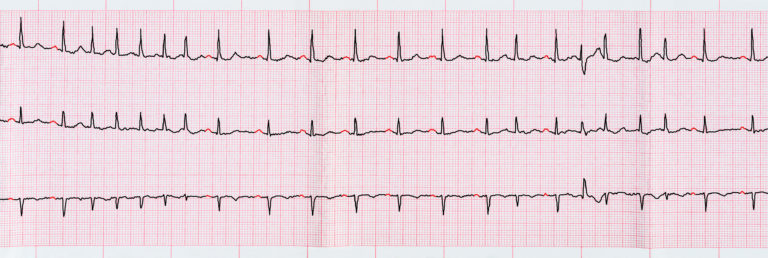
ECG with short paroxysms of atrial fibrillation
Amanda Changuris: Why is AFib so concerning? What can happen as a result of that fluttering feeling?
Dr. Amit Thosani: There are two main risks related to AFib. First and most importantly, AFib increases the risk of stroke, which is our biggest concern. Secondly, symptoms caused by AFib can reduce a patient’s quality of life.
Amanda Changuris: From what I understand, there are a few varieties of atrial fibrillation. Can you describe those for me?
Dr. Amit Thosani: Atrial fibrillation can have a number of different patterns:
Generally speaking, when people first are diagnosed with atrial fibrillation, they tend to be paroxysmal and over time the episodes become more frequent. Often, the individual episodes may become longer in duration or more symptomatic until the point where AFib becomes persistent and stays unless treatment is offered to restore the heart’s normal rhythm.
Our study of the natural history of AFib and treatment outcomes shows that there is likely a time period in which people respond better to treatment, either when they are paroxysmal or early in the persistent stage. However, many patients who are persistent or long-standing persistent may still benefit from restoration and maintenance of normal sinus rhythm.
Jimmie (patient of AHN Cardiovascular Institute): This had to work. That’s what was going through my mind.
Michael (patient of AHN Cardiovascular Institute): I felt that I was sliding into a dark place in my life.
Alexis (patient of AHN Cardiovascular Institute): I wouldn’t have had surgery. I wouldn’t have had this internal device put in. I don’t know what else would have happened if I didn’t meet him.
Dr. Amit Thosani: What we do matters for patients in a life or death situation. So you have to be on every time. I know that everything is going to happen the right way, in a few seconds — you’re about to watch it.
Dr. Stephen Bailey: AGH has a decades long history of leadership and innovation in terms of advancing cardiovascular techniques and procedures. We couldn’t be more appreciative of the collaboration and the support of the Mario Lemieux Foundation.
Caitlin Phalunas: The 2019 gift was very exciting — we were able to pretty much start our electrophysiology research program with that.
David Holmberg: With this gift, what we’re going to do for the health of the entire region is to build a championship program. And this is just the beginning of the investment.
Dr. Emerson Liu: Electrophysiology is a field that intersects a lot of the patient’s other medical conditions, and the treatments range from medications to procedures to implantable devices.
Tom Grealish: Dr. Thosani and his team have created a culture of teamwork, and it’s not surprising that it relates to us. Our chairman was a team player. He was a team owner. He understands the importance of teams working collaboratively, together.
Jimmie: I met Mario the first time, I talked about having AFib, and I would just like to say thanks to him. Because of his generosity, all of us are going to have better lives.
My PCP found out that there was an irregular heartbeat. The hardest part for me was Jada, because we had just lost my wife, so I’m a single parent, and I did not want to leave her.
Dr. Amit Thosani: Jimmie has done remarkably well after undergoing catheter ablation and really is an example of the impact that we’re fortunate to have for many of our patients in improving their quality of life.
Jimmie: My body is back to being the way it should be, and I plan on being around for a long time.
Dr. Amit Thosani: Alexis had an event that has been really in the public’s eye. Everyone knows what happened to Damar Hamlin, and less than 10% of patients who have a cardiac arrest survive, and Alexis is one of those survival stories.
Alexis: I woke up that day, I was 36 weeks pregnant. I went to school, I was feeling great. Before I knew it, I woke up in Forbes.
The doctors alerted me that I went into cardiac arrest at school. Our school nurse performed CPR and used an AED to bring me back to life. They decided it was time to induce me and bring Dominic. December 15th he came into the world. That’s when Dr. Thosani came in and said we’re going to come up with a plan and then by December 18th I was being discharged thanks to Dr. Thosani. I was a new mom leaving the hospital with a brand new baby. I had him to worry about as well as myself, and Dr. Thosani really helped my family and I feel safe and secure.
Dr. Thosani had us buy an AED for our house, so this is my own personal device.
I keep messing this up. This is real. It’s as real as it gets.
Tom Grealish: Putting this money with Dr. Thosani and his team and AHN is going to help with the recruitment and retention right here in Pittsburgh. They make giving easy.
Caitlin Phalunas: I wouldn’t have come to AGH without it. It really has made it a better place for patients. And for my life. You’re going to make me cry.
Michael: I had always been a high-energy person and all of a sudden, even my grandchildren pointed out, gee buddy, why are you just sitting in a chair? You never sit in a chair. I feel lucky because I’ve gotten to meet this team at the Cardiovascular Institute.
Jimmie: They always say, hey Jimmie, how’s it going, how’s Jada, how’s this, how’s that — it’s more like a family.
Dr. Amit Thosani: The way we care for each other in addition to our patients, the way that we are not satisfied with stagnation — we always want to be better than we were yesterday, delivering the type of care that you’d want for your family members. There’s nothing more important to me than that.
Amanda Changuris: Evaluating and reducing a patient’s stroke risk sounds like a top priority for treatment. How do you start that process?
Dr. Amit Thosani: Our first step involves assessing a patient’s risk of stroke, which depends not only on having AFib, but also on other cardiovascular risk factors; for example, heart failure, hypertension, prior stroke or diabetes. After assessing a patient’s individual stroke risk, we may recommend treatment with a blood thinner to reduce the risk of stroke. Blood thinners, also known as anticoagulants, include warfarin or other standard medications that are available — rivaroxaban (Xarelto), apixiban (Eliquis), dabigatran (Pradaxa) or edoxaban (Savaysa).
Warfarin has been used for years, has been proven to be effective, is inexpensive, and for many years was the best available option we had for reducing stroke risk related to AFib. One challenge, however, is that it’s often difficult to maintain warfarin in what we call the therapeutic range. We want it to keep the blood thin enough to reduce the risk of stroke without significantly increasing the risk of bleeding. In our best clinical trials, the time that patients who take warfarin are in the therapeutic range is usually at best about 60%. That means that up to 40% of the time, patients may not be adequately anticoagulated and thus not adequately protected from the risk of having a stroke. Warfarin also interacts with different foods and medications, and individual doses must be tailored to each patient.
The other medications I mentioned work differently and their blood thinning effect is much more predictable, which means that unlike warfarin, they don’t require frequent blood testing. They also tend to have fewer drug interactions.
Another advantage is that the risk of a bleeding type of stroke — bleeding in the brain — is lower with the other medications than it is with warfarin. There’s still a risk of bleeding on any blood thinner, but the lower risk of a bleeding type of stroke is an important consideration.
Amanda Changuris: Once you’ve addressed a patient’s stroke risk, what’s next?
Dr. Amit Thosani: Patients often seek treatment because the symptoms of atrial fibrillation result in a decreased quality of life.
We have been fortunate to build a comprehensive Center for Atrial Fibrillation, which has evolved into the Mario Lemieux Center for Heart Rhythm Care. Our program consists of talented cardiac electrophysiologists, cardiac surgeons, nurse practioners and specialized technical support staff. We strive to provide personalized care for each of our patients, and we are always available.
We can offer various treatment options for patients suffering from symptoms due to AFib, which range from medications to help control the heart rate, to stronger medications called antiarrhythmic medications, which help control the heart rhythm, to procedures to restore and maintain a normal heart rhythm.
One such procedure is called a cardioversion. A cardioversion restores the heart’s normal rhythm with a controlled electric shock while the patient is asleep. In some cases a cardioversion can be performed with medications without an electric shock. We also offer more advanced treatment options known as AFib ablation procedures, which are designed to minimize the risk of recurrent atrial fibrillation by eliminating the triggers and, in some cases, the substrate for the arrhythmia.
Amanda Changuris: What are those triggers?
Dr. Amit Thosani: The most common reason people have atrial fibrillation is because of triggers from structures called the pulmonary veins.
The job of those pulmonary veins is to return oxygen-rich blood from the lungs to the heart so the heart can pump it out to the body. The pulmonary veins contain muscle sleeves that can fire at random and set the heart off its normal rhythm.
This physiology is the foundation for our ablation procedures. We use either radio frequency energy or cryoablation — freezing the veins — to electrically uncouple those veins so when they are active and firing, they don’t disrupt the heart’s normal rhythm.
Amanda Changuris: Does AFib often occur alongside other health issues or conditions?
Dr. Amit Thosani: Atrial fibrillation is associated with a number of issues. Obesity is one, obstructive sleep apnea — which is a treatable condition — is another driver of atrial fibrillation. Other risk factors include high blood pressure, coronary artery disease, valvular heart disease, diabetes and lung disease. Some patients may not have any of these risk factors but still have atrial fibrillation.
Amanda Changuris: So if I have that kind of history or condition, I’ll want to be extra aware of AFib. Are there steps I can take to reduce my risk even if I’m relatively healthy?
Dr. Amit Thosani: Maintaining a healthy lifestyle for general cardiovascular health is important, not just for preventing atrial fibrillation but other forms of heart disease, as well.
As with many medical conditions, disease prevention is the best way to avoid the need for treatment. Be sure you have a primary care physician, have your recommended medical checkups, and maintain a healthy diet and lifestyle.
 Dr. Amit Thosani is director of Cardiac Electrophysiology for AHN and vice chair for the AHN Cardiovascular Institute. He is also an associate clinical professor at Drexel University School of Medicine. Dr. Thosani specializes in care for patients with heart rhythm disorders. He is an active clinical researcher and is widely published in professional journals.
Dr. Amit Thosani is director of Cardiac Electrophysiology for AHN and vice chair for the AHN Cardiovascular Institute. He is also an associate clinical professor at Drexel University School of Medicine. Dr. Thosani specializes in care for patients with heart rhythm disorders. He is an active clinical researcher and is widely published in professional journals.
He earned a medical degree from Columbia University College of Physicians and Surgeons and completed a residency at Columbia University in New York City. He also completed fellowships in clinical cardiology and clinical cardiac electrophysiology at Beth Israel Deaconess Medical Center, Harvard Medical School in Boston, Massachusetts.
Dr. Thosani is board-certified in clinical cardiac electrophysiology and cardiovascular disease by the American Board of Internal Medicine.
You can listen to Dr. Thosani discuss cardiac electrophysiology in this episode of AHN MedTalks.



Highmark Health and its subsidiaries and affiliates comprise a national blended health organization that employs more than 42,000 people and serves millions of Americans across the country.
Entire contents © Highmark Health. All Rights Reserved.
Highmark Health is an independent licensee of the Blue Cross Blue Shield Association.

 Need to find info about providers, prescriptions, coverage, claims, ID cards, or health spending or savings accounts? If so, your Highmark member site is the place to go. (It’s separate from this blog.)
Need to find info about providers, prescriptions, coverage, claims, ID cards, or health spending or savings accounts? If so, your Highmark member site is the place to go. (It’s separate from this blog.)