
 Share This
Share ThisIn our Ask a Doc series, we sit down with physicians and other clinical experts, including those at Allegheny Health Network (AHN), for a chat on an important health topic. In this edition, we’re talking with Dr. Sherif Rizk about surgical options for patients with ulcerative colitis.
About 38,000 Americans will be diagnosed with ulcerative colitis this year alone, with the number of cases approaching 1 million people. The condition is slightly more common in men and is most often diagnosed when patients are between the ages of 15 and 35.
The first line of attack for this painful condition is medication — often antibiotics or biologics such as vaccines or blood products. But in cases where the often grueling symptoms can’t be controlled, patients may want to consider surgical options.
Amanda Changuris (AC): Dr. Sherif Rizk, as an experienced colorectal surgeon, can you tell us what ulcerative colitis is and what symptoms patients experience?

Dr. Sherif Rizk (SR): Ulcerative colitis is a form of autoimmune disease. The body looks at the normal mucosa in the colon as an enemy and attacks it like it would attack an intruder. That leads to inflammation.
The major symptom is bloody diarrhea, and there are other secondary symptoms that go along with that such as poor nutrition, sometimes dehydration, and a general feeling of malaise. Generally, people with ulcerative colitis feel lousy.
AC: Kaitlyn Berkebile, a patient of Dr. Rizk’s, knows just how lousy it feels. She was diagnosed with ulcerative colitis during her freshman year of college.
Kaitlyn Berkebile (KB): The bathroom was pretty much my home for quite a while there. Every time I would eat or drink anything, it would go right through. I had no energy and I was incredibly weak.
Several times before the surgery, I was admitted into the hospital for dehydration. I couldn’t keep myself hydrated, I couldn’t keep myself nourished. It was a very unpleasant state.
KB: I talked to Dr. Rizk and I knew that surgery was somewhere in the near future because unfortunately the medications were not going to work.
So he explained the surgery and one thing that was very, very helpful was that he did a lot of drawings on the exam table paper to map out and help me understand the process. This was all new to me and I didn’t have time to research it and [before that] I didn’t understand very much.
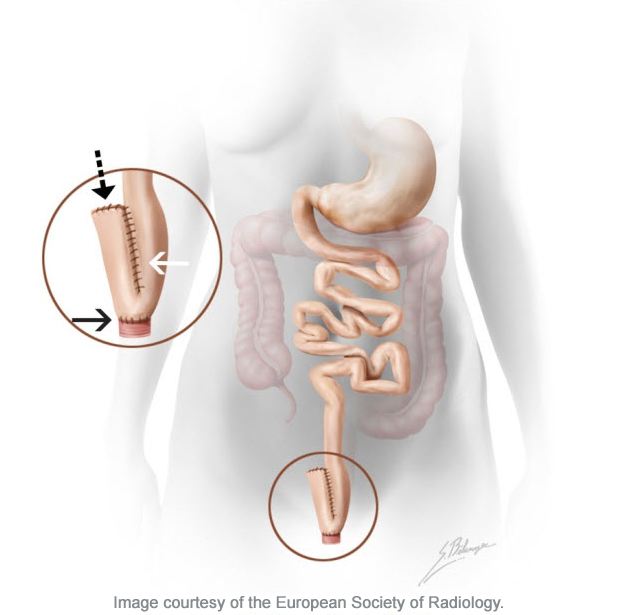
SR: In surgery, we remove the entire colon, which is the target the immune system attacks. That means we remove the abdominal colon and the portion of the rectum that lies in the abdominal cavity and the pelvic rectum down to what we call the anorectal junction (pictured in red below).
Then we take the small bowel and we form a J — as in the letter J — shaped pouch in an effort to replicate the normal rectal reservoir that we have removed surgically (magnified below). Then we connect that reservoir to the anal canal.
AC: The process is completed in a series of surgeries over several months to allow the patient to heal and recover between procedures. Dr. Rizk, can you walk us through those stages?
SR: When the procedure is performed in two stages, we do all of the removal at once. We construct the pouch at the same time and connect the pouch and the anal canal. And we go up higher, above the pouch, and we bring down a temporary diverting loop ileostomy.
Then we allow all surgical staples and suture lines to heal and come back three to six months after the initial procedure and reconnect the small bowel to allow the food that we eat to go down into the stomach, through the small bowel, into the J-pouch and out of the anal canal.
In a three-stage procedure, which is usually done in an emergent or urgent situation, the most immediate concern is to either treat a perforated colon or to keep an imminent perforation from happening. In those situations, the objective is to remove the severely diseased portion of the colon down to the colorectal junction and leave a portion of the pelvic rectum in place and close that off so we can come back at a later date and construct the pouch.
The benefit of this approach is that we remove the immediate, life-threatening piece of the colon and then preserve the rectum for reconstruction when the patient is in much better shape, and a generally improved state of health and nutrition.
AC: Just a few days after discussing her surgical options, Kaitlyn found herself going in for an emergency surgery and expecting a three-stage procedure.
KB: I couldn’t wait any longer. I had wanted to wait until I was finished with that semester of school, but unfortunately that wasn’t going to happen. It was April 1 when I had the first surgery. I had the second stage in June and they were able to do the third stage at the same time. We originally thought it would be three surgeries, but they were able to do it in two which was awesome. I didn’t have to deal with the [ileostomy] pouch for much more than a few months.
SR: Once the final stage is completed and the patient goes through the recovery period, which is typically six weeks or even longer considering the magnitude of the surgery, the majority of patients are very happy.
KB: I was terrified at first, without a doubt, but I couldn’t be happier with where I am right now. The quality of life I had before was not too enjoyable and limited a lot of what I could do, but now I’m pretty much free to do whatever I want. I have a few dietary restrictions, but other than that everything is going very, very well.
AC: And what about school? Were you able to get back on track?
KB: It was my sophomore year when I had the surgery in April and classes weren’t over until May. Waynesburg University let me finish the semester from home after I had a chance to recover from surgery, take all of my exams and everything, and that following fall I did return.
AC: Kaitlyn was a valedictorian of her graduating class and just finished her first year as a teacher in Somerset, PA. And while she’s enjoying the shorter-term benefits of her surgery, Dr. Rizk is also assessing the long-term benefits for her and other patients like her.
SR: Ulcerative colitis in particular and inflammatory bowel disease in general increase the risk of colon cancer quite a bit, so the bonus of this procedure is that by removing the colon we’ve also eliminated the majority of the potential for the development of colon cancer.
AC: While surgery is an effective option for patients with ulcerative colitis (studies point to a 93-percent success rate), the procedure is still relatively rare. Dr. Rizk and his colleagues estimate they do 25-35 J-pouch surgeries each year.
For patients who aren’t able to manage their symptoms using medication, like Kaitlyn, surgery can drastically improve their quality of life.
 Dr. Sherif Rizk is a colorectal surgeon at Allegheny General, Forbes and West Penn Hospitals in Pittsburgh. When he’s not at the hospital, Dr. Rizk enjoys skiing, boating and photography.
Dr. Sherif Rizk is a colorectal surgeon at Allegheny General, Forbes and West Penn Hospitals in Pittsburgh. When he’s not at the hospital, Dr. Rizk enjoys skiing, boating and photography.



Highmark Health and its subsidiaries and affiliates comprise a national blended health organization that employs more than 42,000 people and serves millions of Americans across the country.
Entire contents © Highmark Health. All Rights Reserved.
Highmark Health is an independent licensee of the Blue Cross Blue Shield Association.

 Need to find info about providers, prescriptions, coverage, claims, ID cards, or health spending or savings accounts? If so, your Highmark member site is the place to go. (It’s separate from this blog.)
Need to find info about providers, prescriptions, coverage, claims, ID cards, or health spending or savings accounts? If so, your Highmark member site is the place to go. (It’s separate from this blog.)