
 Share This
Share ThisHelping people in times of need is part of the job description when you work for a national health and wellness organization, but it’s also interesting to learn how employees carry that desire to help others beyond their jobs.
Allegheny Health Network (AHN) clinical training specialist Jim Stupar is a prime example. In addition to serving as a paramedic since 1985, Stupar has been a Disaster Medical Assistance Team (DMAT) member for more than 20 years. Coordinated by the National Disaster Medical System, a joint partnership of the Departments of Health and Human Services, Homeland Security, Defense, and Veterans Affairs, DMATs include doctors, nurses, paramedics, and other medical specialists deployed by the federal government to provide medical care during natural disasters and other events.
Stupar has been on the front lines of medical treatment missions after some of the nation’s worst disasters. In 2017, he was one of several AHN employees who served on DMAT teams after Hurricanes Harvey, Irma and Maria. No doubt, he’ll be serving somewhere again in the months ahead, but meanwhile he took a moment to talk with me about DMAT service.
Corey Florindi (CF): Unless they’ve been in a disaster or know someone like you, people might not realize that DMATs even exist. How would you describe what it means to be on a DMAT?
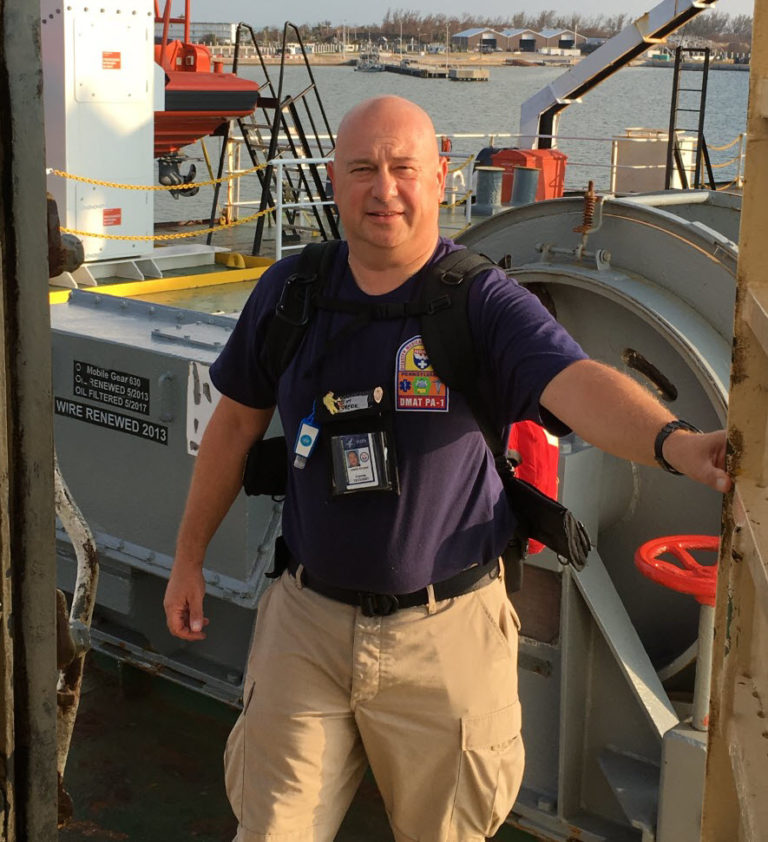
AHN training specialist Jim Stupar aboard a merchant marine vessel where he was quartered during a relief mission in Key West after Hurricane Irma.
Jim Stupar (JS): DMAT members are basically at-will employees of the federal government who are only employed when there’s a disaster or crisis. It’s similar to the National Guard. We have other full-time jobs, but when a disaster occurs, we can be activated and deployed as federal employees to a specific zone where aid is needed.
DMATs include nurses, doctors, paramedics, respiratory therapists — a wide range of medical professionals. We have our regular day-to-day health care jobs, in various settings, and different regions, but we come together and work as a team in that disaster setting.
CF: How long does a DMAT activation last?
JS: The average is two weeks, but the intensity of the needs can make it longer. We had two people who deployed as part of relief efforts for Hurricane Irma in Florida, and then were asked to go from there to Puerto Rico to help with the response to Hurricane Maria, so they ended up being away from home for five weeks.
CF: What is a DMAT set-up like — are you working out of tents, or do they put you in the nearest working medical facility?
JS: It depends. Sometimes we’re setting up mobile tents brought in on tractor trailers. We take them out of boxes and crates and literally build our medical care center when we arrive. That may be in a parking lot, a football field, wherever there’s room.
Another option is using a designated shelter like a gymnasium. You could set up inside a gym and then you might be responsible for providing care to a specific group, like people bussed in from a nursing home that’s lost power, for example.
Logistically, you need to be able to get trucks and ambulances in and out. The ground itself is always a huge factor. Is it firm? Is it marshy? Do we have concrete roads? Is there space for a landing zone if we need to fly people in or out? That’s critical.
After Hurricane Irma, we set up in a parking lot across the street from a local hospital that had to shut down during the storm. During Hurricane Matthew in 2016, we set up in the parking lot of a hospital and took some of their patients so that hospital employees could take a break to go home, be with their families, and assess their own property damage.
CF: Are you activated and deployed with the same group of people from your region?

Jim provided support to another DMAT during ongoing relief efforts in Puerto Rico.
JS: It’s 50/50. You have four on-call months that you sign up for each year, and then you go out with whomever from your team is available at a given time. But sometimes they put you on another team if there’s a need. I went to Puerto Rico with a different regional team. We call that a backfill — a team that’s up for service may not have enough people to meet the need in a given area, so then they ask or assign people from other teams.
Additionally, we sometimes work with other agencies. During Hurricane Irma, the Merchant Marines sent down a ship with FEMA Corps members, for example. So, we often serve alongside others as well.
CF: When you get deployed, how much notice do you receive?
JS: If we’re on call, we’re expected to always be packed and ready to go at a moment’s notice. If you have a category 4 or 5 hurricane and it’s headed toward populated areas, we start preparing. In terms of the official DMAT system, you go from alert status to activated status generally in around 24 hours, which is partly a courtesy to your employer. But if it’s a national disaster, you may be activated with less notice. Allegheny Health Network is great at understanding that.

Jim and other DMAT members on their way to help aboard an Air Force C17.
With Hurricane Irma, half of our national DMATs had already been sent to the Houston area to help with Hurricane Harvey. Those of us who were left were ready to go to Florida and we were on alert status for about a week as they tracked Irma. My boss kept saying, “Why are you still here?” Lo and behold, in the middle of a team meeting, my status changed to activated and I left the next morning.
With the earthquake in Haiti there was no notice. Unlike a hurricane, we can’t track the approach of an earthquake for days in advance. I’d been working the night shift, so I didn’t even know there had been an earthquake until I was at a meeting with my son’s principal and he asked about it. Prior to that, DMATs didn’t go international, so I didn’t think I would be going anywhere. But by the time I got home from that meeting, my phone was ringing. I was going to Haiti.
CF: I was intrigued when I saw Haiti listed as a place you’ve served with your DMAT. Is it unusual to get involved outside the U.S.?
JS: Yes, Haiti was due to the magnitude and severity of the earthquake, all the death and destruction, but there are multiple factors that make an international mission rare. The earthquakes in Italy, for example, were severe, but European countries have their own first responders, the military and the Red Cross, so it wouldn’t make sense to send us. A country like Haiti might request aid from the U.S., because they don’t have the same resources.
CF: I’m guessing every DMAT experience is memorable, but can you share your impressions on a couple? What about Hurricane Irma?
JS: We were stationed at a hotel at Disney World during Hurricane Irma. The storm came right over us. Disney World is meant to withstand a category 4 or 5 hurricane, so we were safe and secure. The day after the storm, we got working, and eventually we went to the Florida Keys. It was about an 11-hour drive and we saw the exact opposite of safe and secure. The islands were totally shut down. Mobile homes were gone, buildings were devastated, tree damage and power outages everywhere. When we got there, we were mainly treating people who either couldn’t or wouldn’t leave the Keys. We addressed some medical problems and trauma, but also some assault victims.
CF: With something like a hurricane — in your experience, why do people stay?
JS: Different reasons. It’s often the elderly, people with health issues, people without transportation, the homeless — people who don’t feel like there’s a place to evacuate to. Others might stay to protect their property. It’s a small portion of people, but that’s often who we help as first responders.
CF: Hurricane Katrina in 2005 was a high-profile relief effort — what was that experience like?
JS: I went to New Orleans two months after Katrina hit. Why not sooner? You have to remember that several parishes (or counties) had been evacuated. It’s a mind shock, but there were very few people where we went other than government employees. As they reopened the parishes and people started coming back, that’s when the DMAT is needed to treat medical issues and trauma, and also the kinds of injuries that occur while people are cleaning up or rebuilding. If we had gone down earlier, we wouldn’t have had anyone to help.

DMAT members must be resourceful to overcome challenges while delivering aid and medical care — but snake handling goes above and beyond.
One thing I remember about New Orleans is that there were snakes everywhere. We had to rattle the portable toilets before we used them because there might be snakes hiding in there. One guy walked in with four snake bites. When he told us where this had occurred, I had to go there and actually find the snake to determine if it was venomous.
The destruction was just terrible everywhere. Collapsed buildings, piles of rubble. I saw a barge stranded half a mile away from the Mississippi River. That’s how far the flood waters stretched when the levee broke.
While we were there, we stayed on a boat on the Mississippi River — a cruise ship brought all the way from Alaska. Typically, we survive on MREs (Meals, Ready to Eat) — one, maybe two, a day and water. With Katrina, we were lucky to get one cooked meal back on that ship each night.
CF: What about Haiti — the earthquake in 2010?
JS: Haiti was the worst of the worst. As we traveled to our camp a day or two after the quake, it wasn’t uncommon to see bodies just waiting to be picked up. Because of all the debris in the air, we often had to wear masks to make sure we could breathe.
In the states we have strict building codes, storm drains, back flow preventers, all these things that help mitigate damage. That’s not always the case in Haiti. You’d have buildings just pancake on top of themselves — three- or four-story buildings flattened. Another difference — in the U.S., you have bulldozers and other heavy construction equipment cleaning up debris relatively soon after a disaster. In Haiti, people were moving debris by hand to help us get through to tend to people in more remote areas.
My DMAT worked out of the base used by the 82nd Airborne, on top of a hill. In the valley thousands and thousands of people were living in a tent city with nowhere else to go. I remember this group of phenomenal Haitian men and women — if a person was sick or injured and couldn’t walk, they carried them up our very steep hill to get treatment.

The baby delivered during the earthquake recovery mission to Haiti.
Food was air-lifted in to distribute. The military would take 20-lb. bags of rice, beans, and grain down the hill. They set up a long tarp down the hillside to slide the bags to the people waiting for food. All of our water had to be brought in on tanker trucks — Haiti didn’t really have any supply of clean water left.
We had a lot of amputations. Normally, that would require an emergency room, but in that type of setting, you just have to triage and treat people in the field. To end on a positive note, a woman came in to one of our tents and told us she was pregnant — and our team helped deliver her baby.
CF: You were also involved in Hurricane Sandy in 2012?
JS: Yes, what’s interesting about Hurricane Sandy is that when we arrived, all the beaches and roads were completely washed away, but we set up tents and got to work. Then a few days later there was a blizzard! We didn’t have shovels or winter coats — we were there to respond to a hurricane! Trying to find a winter coat in the middle of a disaster zone was a challenge.
CF: In terms of disaster response and relief, where do you see room for improvement?
JS: Mostly logistics. How can we get DMATs and responders to impacted areas sooner with a clear mission so we help people that need us as soon as possible? It’s frustrating watching the news from your hotel room or airport because you’re not able to be there and set up yet.
CF: From the other side — what can people do to better prepare themselves for disasters?
JS: You don’t have to be a doomsday prepper, but it is smart to prepare for the possibility of a disaster. Typically, the federal government isn’t able to respond until 36 to 48 hours after the event is over, so you should have supplies to last at least that long: one gallon of water per person, per day; canned or packaged food that won’t spoil; batteries; extra medications if appropriate. It’s important to at least cover the basics. It also doesn’t hurt to read up on what to do when a disaster hits. The federal government has a good online resource that explains what items you should place in your emergency preparedness kit. Being informed and prepared can get you through some hard times.



Highmark Health and its subsidiaries and affiliates comprise a national blended health organization that employs more than 42,000 people and serves millions of Americans across the country.
Entire contents © Highmark Health. All Rights Reserved.
Highmark Health is an independent licensee of the Blue Cross Blue Shield Association.

 Need to find info about providers, prescriptions, coverage, claims, ID cards, or health spending or savings accounts? If so, your Highmark member site is the place to go. (It’s separate from this blog.)
Need to find info about providers, prescriptions, coverage, claims, ID cards, or health spending or savings accounts? If so, your Highmark member site is the place to go. (It’s separate from this blog.)